
Blog
Leadership, Burnout,
and the Realities of Work
Practical posts drawn from healthcare leadership,
coaching, and real-world experience.
The Workforce Has Shifted: Why Burnout, Workplace Stress, and Leadership Matter More Than Ever
For years, many leaders operated under a simple assumption: most employees were doing okay, and only a small percentage were truly struggling.
For a long time, the data supported that belief.
But something has changed in the last few years.
A Turning Point in Workplace Wellbeing
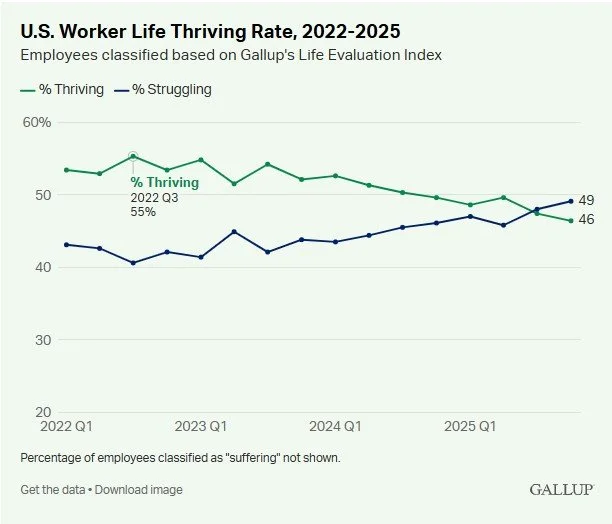
Until 2022, data from Gallup consistently showed that a majority of U.S. workers described themselves as thriving, while a smaller percentage reported struggling or suffering in their lives and work.
By 2023, when I began speaking more frequently on workplace burnout and employee wellbeing, those lines were moving in the wrong direction—fast.
They were on track to cross for the first time.
And now, they have.
In 2026, more U.S. workers report that they are struggling or suffering (54%) than thriving (46%). That’s not just a statistic. It’s a signal of a workforce under sustained pressure.
Burnout, Job Dissatisfaction, and a Stuck Workforce
The implications go beyond engagement scores.
More than half of U.S. employees are actively looking for a new job
Yet only 28% believe it’s a good time to find a quality job
Workers feel stuck, discouraged, and increasingly burned out
This is where workplace burnout, job dissatisfaction, and chronic stress collide.
Employees aren’t just unhappy. They are trapped.
And that creates a dangerous combination for organizations:
low morale, declining productivity, disengagement, and high turnover risk.
Why Traditional Solutions to Burnout Are Falling Short
So how are many organizations responding?
Perks.
Pizza parties. Bonuses. Small morale boosters.
To be clear—compensation and appreciation matter. No one is turning those down.
But they are not solving the core problem.
Burnout is not a pizza problem.
And it’s not primarily a pay problem.
It’s a leadership and workplace culture problem.
The Real Solution: Leadership Development and Workplace Culture
If the workforce has changed, leadership must change with it.
Today’s employees need more than direction—they need support, clarity, psychological safety, and leaders who understand the human side of work.
That means investing in leadership development, emotional intelligence, and people-first management skills.
Managers are not just task supervisors anymore. They are culture carriers.
They have the greatest influence on whether employees:
feel supported or isolated
stay engaged or mentally check out
remain in their role or start planning an exit
When you improve leadership, you improve the entire system.
The Overlooked Reality: Leaders Are Burned Out Too
There’s another layer many organizations miss:
Leaders themselves are struggling at similar levels.
They are navigating:
increased expectations
constant change
emotional load from supporting their teams
pressure from senior leadership
This is why leadership development has a double impact:
it supports the leader and every employee they manage.
Building a Workplace Where Employees Can Thrive Again
If more than half your workforce is struggling, incremental fixes won’t work.
Organizations that want to stand out—those that want engaged, loyal, and thriving employees—must take a different approach.
They must:
prioritize workplace wellbeing
invest in leadership skills, not just technical skills
create psychologically safe and supportive environments
treat burnout as a systemic issue, not an individual weakness
The organizations that do this well won’t just survive this shift.
They’ll become the exception.
A Different Kind of Workplace Is Possible
Right now, most organizations are dealing with a workforce that feels burned out and stuck.
But it doesn’t have to stay that way.
With the right leadership development strategy, you can create a workplace where people:
feel valued
stay engaged
and actually thrive
If you’re ready to invest in your leaders and build a healthier, more sustainable workplace culture, let’s talk.
Want to go deeper?
You can explore the full data and trends directly on Gallup’s site.
10 Ways to Make Orientation Burnout-Proof (Especially in Healthcare and Human Services)
Burnout doesn’t start six months into the job. The stage is set from day one.
Orientation and onboarding are supposed to help new employees feel prepared, supported, and connected to purpose. Too often, they do the opposite—information overload, emotional whiplash, or silence around the parts of the job that are actually heavy.
Whether you work in healthcare, education, nonprofits, or any people-centered field, the way you welcome new staff can either prevent burnout or accelerate it.
Here are 10 ways to make orientation a foundation for resilience—not exhaustion.
1. Shadow First, Train Second
Before handing someone a binder and a login, let them watch real work. Shadowing helps them connect policies to purpose, instead of drowning in procedures they don’t understand yet.
2. Pair Them with a Real Mentor—Not Just a Cheerleader
Assign a peer who will tell the truth. Someone who knows the job, remembers what it’s like to be new, and doesn’t pretend everything is perfect. This builds trust faster than any handbook.
3. Normalize Moral Distress from Day One
Especially in healthcare, social work, education, and ministry. Say it out loud: “Some days, you’ll know the right thing to do and won’t be able to do it. When that happens, here’s who you talk to.”
Naming it prevents shame and isolation later.
I mandated new coworkers to see a therapist after 90 days on the job—to normalize the need.
4. Explain How to Speak Up—And What Happens When They Do
Don’t just say, “We value feedback.” Tell them the exact process for reporting concerns, who will respond, and how they’ll be supported. Uncertainty breeds silence. Silence breeds burnout.
Most people need to be incentivized to speak up, and reassured that it’s expected.
5. Build in Reflection Time, Not Just Training Time
Most orientations are a firehose of information. Add 5–10 minutes at the end of each section with questions like:
What surprised you today?
What felt heavy?
What do you still need to know to feel ready?
Reflection helps them process instead of just absorb.
6. Teach Them How to Use PTO—Not Just How to Request It
New staff need to hear: “You are expected to rest. You don’t have to be exhausted to use your time off.” Better said in month one than year three.
7. Show Them What “Good Work” Looks Like Here
Not the poster version—the real version. Invite a respected employee to talk about a moment they were proud of, and a moment they struggled. This builds identity and purpose. People want to know how they can “win” at work—what qualifies as a job well done.
8. Introduce the Emotional Support System, Not Only the IT System
Most orientations explain payroll, passwords, and parking. Very few explain where to go when the job hurts emotionally. Provide names, email addresses, chaplains, employee support teams, wellness programs—real people, not just vague reassurances.
9. Let Them See Wins Early
Give a small, meaningful task they can complete in the first week. Let them contribute instead of just observe. Purpose is a burnout buffer.
Praise them for the tiniest positive actions—it communicates values.
10. Ask How They’re Really Doing (Before It’s Too Late)
Three to four weeks in, check back. Not with “How’s it going?” but with:
What’s harder than you expected?
What’s going well?
Where do you need support?
Catching burnout early is a leadership skill.
Want to Know How Burned Out Your Team Already Is?
Before fixing orientation, measure what staff are actually experiencing.
You can take or share my free burnout test here: MyBurnoutTest.com
Need Help Building This into Your Culture?
I work with hospitals, schools, nonprofits, and companies to build orientation and leadership practices that prevent burnout—not just respond to it.
You can explore speaking and workshop options here:
https://patrickriecke.com/live-presentations
Or, for self-paced team tools, scripts, and reflection guides, visit:
https://www.myburnouthub.com/learn-more
15 Low-Cost Ways to Reduce Burnout (That Work Better Than Pizza Parties)
You can’t cure burnout with cupcakes or a nacho bar in the break room.
Most employees aren’t desperate for snacks or swag. They’re desperate for manageable workloads, a voice in decisions, and a workplace that treats them like people—not machines.
Here are 15 meaningful, low-cost ways leaders are actually reducing burnout. No balloons. No “wellness carnival.” Just real changes that make work more human.
1. Quiet Hour (No Meetings, No Messages)
Block one hour each week for protected work time. No meetings. No chat notifications. Don’t just suggest it—defend it.
2. Peer Coverage for Actual Breaks
Instead of “take a break if you can,” build a simple coverage plan so people can walk away without guilt or chaos.
3. Rotate Emotional Labor Jobs
Some people always handle upset families, angry customers, or grieving patients. Rotate these roles or give those staff time to recover afterward.
4. “No-Reply Fridays” or Email-Free Windows
One day or one morning a week with no internal emails or non-urgent messages. Teach people to pause before pressing send.
5. Stop Rewarding Overwork
Don’t celebrate the employee who stays until 9 p.m. Celebrate the one who finishes on time and still delivers quality.
6. Let People Say ‘I Don’t Know’ Without Fear
Psychological safety reduces burnout more than any wellness challenge. Admitting uncertainty shouldn’t be a career risk.
7. Give Schedule Input, Even in Small Ways
Let people choose between early/late starts, trade shifts, or block certain hours for focused work. Autonomy is fuel. [Not always possible, but sometimes overlooked when it is]
8. “What Should We Stop Doing?” Meetings
Once a quarter, ask the team which tasks, meetings, or reports are wasting time. Then actually eliminate one.
9. Fix One Broken Workflow
Pick the process everyone complains about—and fix it. Don’t make employees work around dysfunction and call it resilience.
10. Give People Real Recovery Days (Not Random PTO)
If someone’s been in an emotionally heavy season—ICU staffing crisis, student crisis, hospice cases—offer one recovery day without making them use vacation hours.
11. Invite, Don’t Assign, New Initiatives
“Who wants to help lead this?” gets better energy than “I put you on the committee.” Choice matters.
12. Ask Better Check-in Questions
Try:
What’s one thing making work harder than it needs to be?
Is anything getting in the way of you doing your job the right way?
Real questions lead to real solutions.
13. Protect Learning Time
Give staff a small window monthly for professional growth—an article, CE module, or leadership video. It tells them growth matters more than constant output.*
14. Leader Walk-Arounds With One Question
Not clipboard checklists. Just one question: “What do you need that you don’t have?” Listen. Respond to their actual needs, not your own guesses.
15. Let People Finish the Work They’re Proud Of
When someone is forced to rush, cancel, or compromise quality over and over, it creates moral distress. Give them time to do it right at least once a week.
Want to Know Where Your Team Really Stands?
Before making changes, measure burnout honestly. You can use my free assessment tool here:
MyBurnoutTest.com
Ready to Build This Into Your Culture?
*These practices come straight from my workshops and the leadership path inside The Burnout Hub—a resource for teams who want to prevent burnout with real strategies, not slogans.
Explore it here:
https://www.myburnouthub.com/learn-more
If you'd like me to train your leadership team or speak at your event, you can check availability here:
https://patrickriecke.com/live-presentations
7 Scripts to Push Back on Overwork (Without Sounding Difficult or Unprofessional)
Most people don’t burn out because they’re weak or uncommitted. They burn out because they never learned how to say, “This is too much,” in a way that doesn’t sound angry, dramatic, or disloyal.
So they say nothing. They stay late. They absorb more. And eventually, they shut down.
You don’t need a perfect boundary speech. You just need language that’s honest, professional, and still human. Here are seven scripts you can adapt when work keeps asking for more than you can give.
1. When You're Given More Work Than You Can Take On
Old response: “Sure, I’ll get it done.” (While panicking internally.)
Try this instead:
“I can take this on. Which project would you like me to delay or hand off so I can give this the attention it deserves?”
This keeps you helpful, but reminds people your capacity isn’t infinite.
2. When the Deadline Is Unrealistic
Old response: “I’ll try.”
Try this:
“To meet that deadline, I would need to set aside other responsibilities. Is the priority speed or quality on this one?”
You’re not refusing—you’re asking them to choose.
3. When You Keep Getting Pulled Into “Quick Questions”
Old response: “No problem!”
Try this:
“I want to help. I’m working on something that needs focus—can I circle back at ___?”
Saying no to interruptions makes space for real work.
4. When You’re Expected to Always Be Available
Old response: “Text me if you need me.”
Try this:
“After 6 p.m., I’m offline unless it’s urgent. If it’s something that can wait until morning, email works best.”
Clear communication beats silent resentment.
5. When You’re Volun-told for Yet Another Committee or Task Force
Old response: “If no one else wants to, I’ll do it.”
Try this:
“I care about this work, but I’m at capacity. If you still need me involved, something else will need to come off my plate.”
6. When Someone Drops a Task on You at the Last Minute
Old response: “I’ll make it work.”
Try this:
“I can do that, but not by today. I can have it to you by ___, or I can help you find someone who’s available sooner.”
7. When You Feel Guilty for Saying No At All
Internal script to practice:
“I am not failing—this is me choosing to stay healthy enough to keep doing good work.”
If you only change one thing, let it be this: boundaries aren’t barriers. They’re oxygen.
Not Sure How Burned Out You Really Are?
Before you assume “this is just how it is,” get a clear picture of where you stand.
Two-minute burnout screening here: MyBurnoutTest.com
Want More Language, Tools, and Support?
This kind of communication is built into The Burnout Hub—video lessons, downloadable scripts, reflection prompts, and leadership tools you can use with your team.
You can explore it here:
https://www.myburnouthub.com/learn-more
Or if your organization needs training, a keynote, or a workshop on burnout and moral distress, my speaking availability is here:
https://patrickriecke.com/live-presentations
The Pitt, Brain Death, and My Repressed Emotions
The Complicated Death of a Teenager
As the brain dead teen laid in the bed, his tattoo arm sleeve still demonstrated his personality. I'll never forget the beautiful images.
Five days earlier, I met his parents in a consult room. At that time, his mom would not accept the news of his brain death.
She begged God for a miracle, and implored us to wait--to leave him on life support.
Waiting is complicated in these situations--when a patient has been declared brain dead.
One complication in this case was that the young man was "donor-designated"--he had a heart ❤️ on his license.
In the state of Indiana that's considered a binding advance directive.
In plain English--he was going to be an organ donor whether mom approved or not.
For days, she did not approve.
Yet, ten days after his car accident, the organ procurement organization was gowned up, standing outside his ICU room, and ready to take him to the operating room.
An honor walk was scheduled for the afternoon.
Then it was pushed back to early evening.
Healthcare Leaders--Always On Call
It was Friday. I was at home. I was not on call. But healthcare leaders know that--in situations like these--it doesn't matter if you are technically on call or not. At 6:30 that evening, my phone rang.
"The mom is refusing to accept the brain death diagnosis--again."
After a long week at work, I didn't bother to put my suit back on. I just grabbed my badge and headed back to the hospital.

"She said she'll throw herself onto his bed if we try to wheel him to the OR for organ recovery..." the nurse leader was working late, too.
At 6:45, I met with the team outside of his room--donor network, nurses, and public safety. They were throwing up their hands, at a loss for what to do next. They were stuck between the need to procure his organs and the possibility of having to physically restrain his mother.
No one wants to be heavy-handed with a grieving mother. Least of all, me.
After all, her son was the same age as one of my own sons. Putting myself in her shoes was easy.
Both our sons were big-hearted, outgoing, faith-focused young men.
The Tug-of-War between Grief and Medicine
The team looked at me--"What are we going to do?"
I assured the representative from the organ procurement agency that we understood--the patient had to donate.
"Can I go into the room?" I asked.
Inside, I hugged his mom. I stood in silence. I asked about his tattoos. We made some connections about our faith, our friends, and being parents.
"Are you 100% sure he is brain dead?" Mom finally choked out her question.
I stayed silent. She wasn't actually looking for answers.
Later, I gently slid the words out to mom, "You asked if we are sure. The answer is yes, we are 100% sure."
Finally, she started to cry.
"No one can say I didn't fight for him until the end..." she surrendered.
"No," I echoed. "No one can say that."
We encircled the young man in prayer. RNs, Nurse Manager, donor network team, family, and me. Tears fell onto the concrete floor. Just as they are falling on my desk and keyboard as I write these words.
The honor walk solemnly began after the long delay. Dozens of family and friends lined the hallways, peppered with staff from our hospital.
When we reached the red and white tape on the floor that designated the entrance to the surgery wing, the procession stopped for the parents to say goodbye one last time.
Even Hell is Filled with Miracles
Nearby, one of our public safety officers stood--quiet and respectful--grateful he wasn't called on to restrain this grieving mother.
Mom spotted a tattoo on the officer's arm--a bright, colorful depiction of heavenly gates. Standing at the surgery threshold after her son was wheeled away, she took his arm in her hands, wiping tears.
She touched the officer's tattoo. Held his arm. He did not pull away. He understood.
As her son entered those gates, it just so happened that an officer stood nearby with this icon blazing across his arm.
Back in the ICU room, now empty, the patient's dad thanked me for coming. He said, "You preserved a lot of peace tonight."
The Incurable Condition of Moral Distress
Yesterday, I read a social media comment that claimed one of the tasks of nursing school is to "spare future nurses moral distress."
Obviously, that is bull sh*t.
As vital as education is, nothing prepares a person for these moments.
Moral distress and moral injury can never be eliminated in healthcare. As long as teenage boys, completely sober, total their cars and end up braindead, there will always be moral distress.
The Pitt and The Truth About Healthcare
That's the end of my story. If you want to discover my reason for writing now, read these last few paragraphs.
I am probably the last person in America to finally start watching the hit series The Pitt.
Season one includes the story of Nick Bradley. A braindead teen boy.
Nick and my patient were similar.

I cried several times while we watched these episodes, and my experience came rushing back like a spring-loaded punch to my face.
Had I repressed this story--this experience of secondary trauma?
Probably.
Why?
Not because it was the hardest experience I witnessed. It wasn't.
It was for three personal reasons:
It was because this patient's death occurred two months after a good friend of mine died during childbirth. I stood in her room when she was also declared brain dead. And my wife and I became primary support people for her widower and newborn baby (that would last for a couple of years).
This patient with the tattoos died one week before my father-in-law died. One of the world's sweetest men, his absence left a huge hole for our whole family.
Finally, this patient died two weeks before my own son graduated from high school.


So, yeah. I probably repressed my feelings about this experience until--years later--it was safe to feel them while watching Dr. Robby navigate Nick Bradley's death.
These morally distressing patient experiences--they never happen in a vacuum. We face them in the middle of our own stories.
Today, healthcare workers are showing up for their patients despite...
Their miscarriage grief still feeling raw
The angst from their last shift trying to pin them to their bed
Their mind looping on the last patient they watched die
Their questions about what good they are doing in this broken and dying world
And, while they work today, something will go wrong. They'll lose a patient. Or be physically assaulted. Or a leader will be overly critical. Or a family member will accuse them of not caring about their patient.
When people talk about moral distress, stress in healthcare, and burnout as something we have to "fix"--it demonstrates that they don't understand.
You don't fix this.
You address it. You acknowledge it. You try to overcome.
But it can't be fixed.
And that. That's why I do what I do.